The thoracic wobble or flapping chest is a rare pathology in childhood . It is the alteration suffered by the rib cage when there is a double fracture of several ribs.
Concept
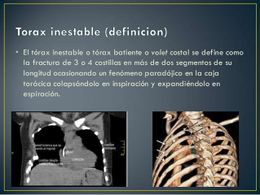
It is called thoracic wobble or flapping chest to the alteration suffered by the rib cage when there is a double fracture of several contiguous ribs , determining loss of rigidity of the rib cage. This results in the fractured area moving freely and in the opposite direction to the movements of the thorax , so that during inspiration the fractured area is depressed and on expiration it bulges, producing serious cardiorespiratory mechanical disorders.
Etiology
The common causes of rib fractures of this type are severe contusions of the chest and crush injuries. Sternum fracture and intrathoracic organ injury frequently occur, worsening the prognosis.
Pathophysiology
The pathophysiological alterations that occur when the fractured area moves freely are due to the fact that during inspiration the intrathoracic negative pressure increases, causing the fractured area to shrink; this causes a decrease in expansion in the lung on the injured side. There is also a mediastinal deviation towards the healthy side because the negative pressure is greater on this side and the phenomenon of the “aiere pendulum” occurs, from the injured side to the healthy side.
During expiration, the fractured area bulges and the mediastinum moves to the injured side, passing oxygen- poor air from the lung of the healthy to the injured hemithorax.
These movements of the mediastinum , called “wobble”, flutter or mediastinal flutter, cause insufficient lung expansion and decreased venous return to the heart.
All these alterations produce marked hypoxia, cardiocirculatory arrest due to hypoxia, and hypovolemic shock due to decreased cardiac output.
Diagnosis
It is based mainly on the history of violent trauma, physical examination, where the paradoxical movement of the fractured area and the chest X-ray where the presence of several fractured ribs is verified.
Treatment
It consists of restoring the stability of the rib cage as soon as possible to prevent the pathophysiological disorders described above from occurring. The affected region is immobilized by different methods: strips of spradic prior to packing with gauze or cotton of the affected area; traction, either of the skin, with silk or erina forceps, or steel wire at the level of the ribs.
Another form of treatment is mechanical ventilation with PPI (Positive Intermittent Pressure) or high-frequency ventilation (HFV). The duration of treatment is never less than 15 to 21 days. Other aspects of the treatment are: analgesics, postular changes, anti-bedsore mattress, adequate nutrition, etc.
Nursing care
- Reception of the patient according to the manual of nursing procedures in Pediatric Intensive Care.
- Grooming if its critical condition allows it; otherwise, it will be postponed until after the emergent measures and improvement of the patient.
- Place the “stop trolley” in a nearby area and ready for use.
- Peripheral vein cannulation with “mocha” or plastic trocar.
- Preparation of the area to perform the deep venous approach as well as the arterial one if indicated.
- Place the patient at 30 degrees to improve respiratory dynamics, partially eliminating the abdominal press.
- Offer adequate oxygenation (tent, chamber, mask, catheter, etc.) until you prepare for intubation and ventilation if necessary.
- Keep the necessary equipment for intubation and ventilation ready if indicated.
- Mobilization of the patient with great care (remember double fractures of several ribs).
- Prepare and assist with thoracic immobilization if required according to medical indications.
- Prepare and carry out methodology for feeding:
- Buccal: Baby bottle, teaspoon, jug.
- Gavage: placement of a nasogastric tube and administration of the agreed feeding.
- Gastroclysis: the same as the previous one, but administering the feeding in a permanent and continuous drip, or discontinuous and cyclical.
- Parenteral: start-up of the infusion pump and preparation of the pertinent solutions for this type of feeding or mixed.
- Monitoring of vital signs.
- Monitoring of the patient’s state of severity and its improvement or progression, for its corresponding report.
- Control and annotation of income and losses to know the hydromineral balance (danger of dehydration or overhydration).
- Care of the bedridden patient in avoidance of bedsores (careful mobilization, use of the anti-bedsore air mattress, keeping it dry, etc.).