It is characterized by a predominance of comprehension disorders, with normal articulation and flow in most cases.
Verbal expression is usually increased, with a certain degree of excitement and ignorance of the defect on the part of the patient. Although oral production is effortless, with good articulation and prosody, unintelligible words predominate (aphasic or paraphasic transformations) that lead to jargon that is difficult to understand and with empty content.
In cases where there is no excessive expression ([logorrhea]), the lack of words is highlighted (anomie). Repeatability and naming are also affected.
The comprehension disorder is the most significant, although with a variable intensity depending on the severity of the injury. For example, the patient understands very poorly what is being said and, although he can express himself, it is difficult to understand due to the use of “strange” or inappropriate words, similar to a foreign language, making it difficult to carry on a conversation
Reading and writing are also impaired. Although there is the ability to write, these patients express themselves in writing as they speak, so writing is often difficult to understand.
Characteristics
- The main characteristic is the difficulty to understand oral and written language and to make sounds legibly.
- He speaks normal although the broadcasts may not coincide with the topic being spoken.
- Presents errors in spoken language, such as phonemic paraphasia (they make sounds or words involuntarily) and anomies (difficulty in naming people, objects or places).
- He repeats, although sometimes he does not understand, what he is saying, or he makes mistakes.
- Literacy is affected, both in the oral emission and in the comprehension of texts.
- They are anosognotic patients; this implies that they are not aware of their difficulty
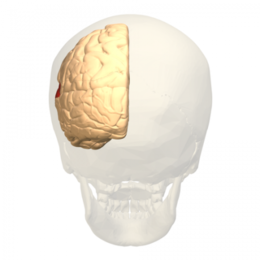
Location of injury
Wernicke’s aphasia is usually due to injury to the posterior two-thirds of the first and second temporal regions. When the lesion encompasses the medial region of the temporal lobe, greater speech deafness occurs, that is, there is a more marked acoustic decoding deficit. If the lesion extends to a large part of the parietal lobe, reading comprehension is more affected.
Signs and symptoms
Patients with aphasia have difficulty understanding written or spoken language and may have trouble expressing themselves well enough for others to understand. There are a number of different types of aphasia. These disorders are classified as either non-fluent or fluent.
Patients who have nonfluent aphasia have difficulty speaking. Some people who have non-fluent aphasia can use only a few words, and others cannot speak at all or cannot understand others, depending on the area of the brain that is damaged. People who suffer from it can speak, but have a lot of conversations difficult to understand. Wernicke’s aphasia is classified as a type of fluid aphasia.
People who have Wernicke’s aphasia don’t always make sense when they speak. They add syllables to words, insertion nonsense words or words that do not apply to the topic and use long, rambling sentences. They are not necessarily aware that their speech is different from other people’s speech patterns, but they often have a hard time understanding what others are saying.
Some people who have this disorder seem to be quick and interrupt others. Most sufferers tend to have relatively normal grammar and can still use complex grammatical structures, but their sentences are meaningless. Many patients replace related words with other words, such as saying “chair” for “table”; others substitute the letters or sounds of familiar words, such as saying “hish” for “fish.”
This disorder can also extend to the patient’s writing. People with Wernicke’s aphasia do not normally suffer from motor coordination problems and are capable of manual skills such as writing, but their writing often resembles the way they speak. They may also have trouble reading, depending on the areas of the brain that are damaged.
Diagnosis
A neurologist or speech-language pathologist diagnoses Wernicke’s aphasia, speaking with the patient and asking him or her a series of questions. You could also give the patient a series of commands to follow or ask the person to name objects. The health care provider determines the severity of the condition based on the patient’s responses.
Therapies and treatments
Patients with Wernicke’s aphasia have a poor prognosis for rehabilitation. Speech therapists work with patients to improve their language skills.
Patients also practice communicating with other people using non-verbal forms of communication, such as face signals and hand signals. As each person presents the disorder differently, the treatment will depend on the affectation and severity that occurs.
Differential diagnosis
It is not surprising that Wernicke’s aphasia is misdiagnosed, as it is easy to confuse with other disorders. A differential diagnosis must first be made with a thorough neurological examination.
This is important because a bad diagnosis will have the consequence that the real problem is treated late or not treated and thus the patient cannot improve.
Therefore, Wernicke’s aphasia cannot be confused with psychotic disorder, since the way of expressing and behaving can be similar, such as incoherence of language or the appearance of disorganized thinking.